 | Idaho Medical Power of Attorney Form |
The Idaho medical power of attorney form is a document that would be executed by someone, known as the Principal to appoint someone else who would be known as an Attorney In Fact or an Agent to oversee the specific wishes of the Principal in their best interest with regard to their medical and health care as if the Principal were available to make their own health care decisions. This document if left blank by the person executing the document shall be deemed to be intentional and shall not invalidate the document. (See Title 39 -Chapter 45 -39-4510.)
Registration – The Principal of the document may choose to file the form with the Idaho Secretary of State (no filing fee required) by completing the Registration Form and sending via mail.
How To Write
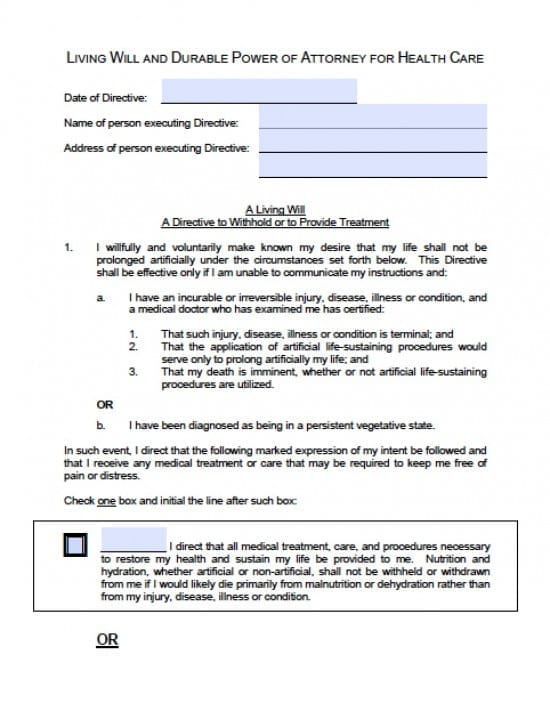
Step 1 – Directive information regarding the Principal – Download the form and begin in section 1 by printing or typing the following information into the lines provided:
- Date of Directive
- Name of person executing Directive
- Address of person executing Directive
Step 2 – The Principal should read the paragraphs with regard to “directives” with their Attorney In Fact/Agent and then check the following appropriate boxes inside of the form as decided by the Principal as follows:
- I direct that all medical treatment, care, and procedures necessary to restore my health and sustain my life be provided to me. Nutrition and hydration, whether artificial or non-artificial, shall not be withheld or withdrawn from me if I would likely die primarily from malnutrition or dehydration rather than from my injury, disease, illness or condition.
- OR
- I direct that all medical treatment, care and procedures, including artificial life-sustaining procedures, be withheld or withdrawn, except that nutrition and hydration, whether artificial or non-artificial shall not be withheld or withdrawn from me if, as a result, I would likely die primarily from malnutrition or dehydration rather than from my injury, disease, illness or condition, as follows: (If none of the following boxes are checked and initialed, then both nutrition and hydration, of any nature, whether artificial or non-artificial, shall be administered.)
- A. Only hydration of any nature, whether artificial or non-artificial, shall be administered
- B. Only nutrition, of any nature, whether artificial or non-artificial, shall be administered
- C. Both nutrition and hydration, of any nature, whether artificial or non-artificial shall be administered
- OR
- I direct that all medical treatment, care and procedures be withheld or withdrawn, including withdrawal of the administration of artificial nutrition and hydration
- I have discussed these decisions with my physician and have also completed a Physician Orders for Scope of Treatment (POST) form that contains directions that may be more specific than, but are compatible with, this Directive. I hereby approve of those orders and incorporate them herein as if fully set forth
- OR
- I have not completed a Physician Orders for Scope of Treatment (POST) form. If a POST form is later signed by my physician, then this living will shall be deemed modified to be compatible with the terms of the POST form
Step 3 – Designation of Health Care Agent – The Principal should read the information provided in this section, prior to appointment of an Attorney In Fact/Agent. Form Definition of “health care decision is as follows:
“For the purposes of this Directive, “health care decision” means consent, refusal of consent, or withdrawal of consent to any care, treatment, service, or procedure to maintain, diagnose or treat an individual’s physical condition.” – Once the Principal has read the information provide the following information with regard to your chosen Attorney In Fact/Agent:
- Name of Health Care Agent
- Physical Address of Health Care Agent
- Telephone Number of Health Care Agent
Step 4 – Statement of Desires, Special Provisions, and Limitations – On page 4 the Principal should carefully read all of the information provided on this page. Once read and understood, place your desires, your wishes for special provisions and any limitations inside of the large box on the following page by print or type. This is a step the Principal will want to take, otherwise, the Agent will be left with broad and sweeping decision which may be made that may not be your true intentions or decisions for yourself – Once you begin providing this information, if you need more room, you may certainly add sheet(s) that may be attached to this form.
Step 5 – Inspection and Disclosure of Information Relating to Physical or Mental Health – The Principal should read all of this section as this is a general grant of authority for your Agent. If there is anything within this section you do not agree with, add a new directive in your special instructions cancelling the directive you do not wish to grant authority over.
Step 6 – Designation of Alternate Agents – Although this section is optional, it is recommended that you select at least one alternate Attorney In Fact/Agent, in the event your original selected Agent becomes unable or unwilling to serve as your Attorney In Fact/Agent. You may select up to three Agents to help with your decisions to be appointed consecutive (one at a time) in the order in which you place them. If you would like to select up to three alternates, provide the following information for each alternate Agent A., B., and C:
- Alternate Agent Name
- Physical Address
- Telephone Number
Step 7 – Signature of Principal – Once you’ve completed all of the information required, at the end of the document you (the Principal) must provide:
- Principal’s Signature
- Date of Signature in mm/dd/yyyy format
- Make copies to provide to each person named as Agent or potential Agent in this document
- Make copies also for any physician or medical facility who may have interest