 | Arizona Medical Power of Attorney Form |
The Arizona medical power of attorney form is a written designation of an agent/attorney in fact to make health care decisions that would meet the requirements of section 36-3221 and that comes into effect and is durable as provided in section 36-3223 Subsection A. This form will allow the principal to grant power to someone that they trust, to make decisions for their health care. As an agent/attorney in fact, this is a very important responsibility. It’s recommended that you speak with your attorney, the principal’s physician and/or clergy before signing this form. It’s also recommended that the principal and attorney in fact/agent, look over the section and subsection with regard to how the law works and what the principal as well as the attorney in fact/agent should expect.
How To Write
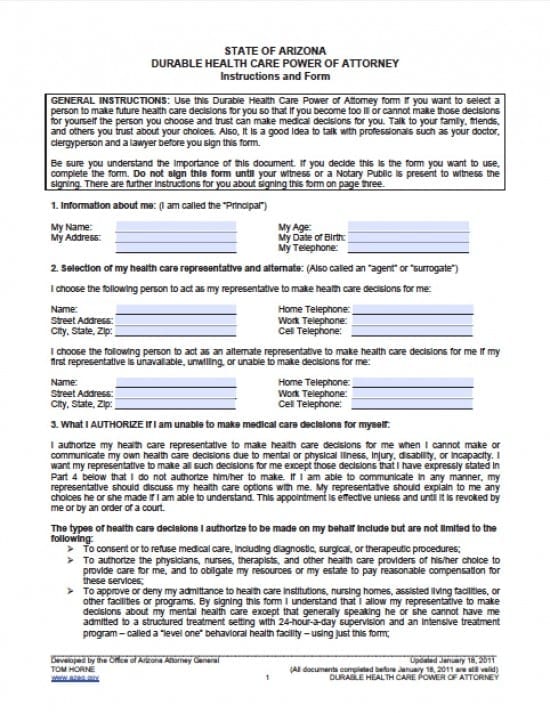
Step 1 – Begin by downloading the form provided and reading the “General Instructions” before proceeding.
Step 2 – Section 1 – Information about the principal – After reviewing the general instructions, the principal will enter the following information about them self:
- Principal’s Name
- Physical Address
- Age
- Date of Birth
- Complete telephone number
Step 3 – Section 2 – Selection of the Principal’s Health Care Representative (attorney in fact/agent) and Alternate – In this section, the principal will enter the information with regard to the first person they would like to name as their attorney in fact/agent. The principal will also provide information with regard to whom they may wish to serve as an alternate agent, in the event the first person is unwilling or unable to act on behalf of the principal for whatever reason. Provide the following:
- First Healthcare Representative’s
- Name
- Physical Address
- City, State, Zip
- Home Telephone
- Work Telephone
- Cell Telephone
- AND
- Alternate Healthcare Representative’s
- Name
- Physical Address
- City,State, Zip
- Home Telephone Number
- Work Telephone Number
- Cell Telephone Number
Step 4 – Section 3 – Principal’s Authorization – In section 3 the Principal must read and understand what this document covers with regard to what rights their healthcare agent’s have. If after you’ve read this information, you don’t understand it, you may wish to consult with an attorney or have the language changed to your preferences – this can be done in the next section.
- Review the paragraphs in section 3
Step 5 – Section 4 – Decisions Principal Expressly Does Not Authorize –
- If there are any aspects of this document that you choose not to authorize, then you may place that information in this section on the lines provided. If there is not enough room, you may add any additional information on a separate sheet to be attached to this document.
Step 6 – Section 5 – Autopsy –
- This section asks that you select whether or not you would like an autopsy performed after death. Make your selection by placing an x before your selection
Step 7 – Section 6 – Anatomical Donations – This section will allow you (the principal) to choose whether or not you would like to donate any or all parts of your body after death. If you make no selections, the person you have elected may do as they believe you would want them to. Select from the following:
- A. I DO NOT WANT to make an organ or tissue donation
- B. I DO WANT to make an organ or tissue donation when I die
- 1. What organs/tissues I choose to donate
- a. Any needed parts or organs
- b. These parts or organs
- If you elect to make specific donations, state them on the lines following your selection
- 2. What purposes I donate organs/tissues for
- a. Any legally authorized purpose (transplantation, therapy, medical and dental evaluation and research, and/or advancement of medical and dental science)
- b. Transplant or therapeutic purposes only
- c. Other (if this is your selection, place your choice(s) on the line next to “other”)
- 3. What organization or person I want my parts or organs to go to
- a. I have already signed a written agreement or donor card regarding organ and tissue donation with the following individual or institution (Name)
- b. I would like my tissues or organs to go to the following individual or institution (Name)
- c. I authorize my representative to make this decision
Step 8 – Section 7 – Burial – This section is optional. If you’ve already made these arrangements you need not complete this section. Otherwise, select from the following subsections:
- My agent has authority to carry out all matters relating to my funeral and burial disposition wishes in accordance with this power of attorney, which is effective upon my death
- My wishes are reflected below: Initial or put a check mark by those choices you wish to select
- Upon my death, I direct my body to be buried. (As opposed to cremated)
- Upon my death, I direct my body to be buried in (place your choice of burial location in the line next to this statement)(Optional directive)
- Upon my death, I direct my body to be cremated
- Upon my death, I direct my body to be cremated with my ashes to be (if this is your selection, state specifically what you would like to have your agent do with your ashes) (Optional directive)
- My agent will make all funeral and burial disposition decisions. (Optional directive)
Step 9 – Section 8 – Living Will – If you have a living will, you must attach it to this document. If you do not have a living will but would like to complete one, ask your physician, agent or attorney to assist you, or create one online. Make the following selection on this form:
- A. I have SIGNED AND ATTACHED a completed Living Will in addition to this Durable Health Care Power of Attorney to state decisions I have made about end of life health care if I am unable to communicate or make my own decisions at that time
- B. I have NOT SIGNED a Living Will
Step 10 – Section 9 – This section will address whether or not you would like to be resuscitated if in fact you do not wish for any added measures to be taken to keep you alive. This should be considered especially if you are terminally ill and there is no hope that you will survive your illness.You may wish to discuss this directive with your family, agent and physician if you have not instructed this directive, prior to making a decision. Make your selection from the following on the form:
- A. I and my doctor or health care provider HAVE SIGNED a Prehospital Medical Care Directive or Do Not Resuscitate Directive on paper with ORANGE background in the event that 911 or Emergency Medical Technicians or hospital emergency personnel are called and my heart or breathing has stopped
- B. I have NOT SIGNED a Prehospital Medical Care Directive or Do Not Resuscitate Directive
Step 11 – HIPPA Waiver – This section will address whether or not you would like your agent to have access to your medical records while they are assisting with your decisions. Make your selections from the following, on the form, by placing your initials in front of the selection if you choose to have your agent access your medical records. If not, leave the line blank:
- I intend for my agent to be treated as I would be with respect to my rights regarding the use and any disclosure of my individually identifiable health information or any other medical records. This release authority applies to any information governed by the Health Insurance Portability and Accountability Act of 1996 (also known as HIPAA), 42 USC 1320d and 45 CFR 160-164
Step 12 – Signature/Verification – Before signing in this section, you must acquire the services of a notary public and one witness to ensure that your rights are being observed. This section will ask you OR your agent to sign this form to verify whether or not you are able to sign the form and if not that all of your wishes are being honored. If you are unable to sign the form, your agent may sign on your behalf. If this is the case, have the paragraph read to you before allowing your agent to sign for you. If you are able to sign on your own behalf, sign the first line and date it.
Step 13 – Signature of Witness and Notary Public – Your witness must provide the following:
- Witness Printed Full Legal Name
- Witness’ Signature
- Date Witness is signing the form
- Witness’ complete physical address
After, the notary public shall complete the execution and affix their seal to the document.
Step 14 – If you would like, you may review the optional paragraph inside of the box with regard to discussions with regard to your healthcare choices with your physician. If you have discussed all of your options and wishes with your doctor, you may have him/her sign stating that they have reviewed this document and understands your choices. Should you have your physician sign this form, the following is required (again, this is optional)
- Doctor’s printed legal name
- Doctor’s signature
- Date the Doctor is signing the document
- Doctor’s full physical address