 | Arkansas Medical Power of Attorney Form |
The Arkansas medical power of attorney form is a document that allows the principal to name a person as having the authority to make medical decisions on behalf of the principal when the specific condition or circumstance occurs. That person is commonly known as a surrogate, an attorney in fact or an agent. The most common conditions or circumstances are when the principal has a terminal illness and is expected to die in a small amount of time or if the principal is permanently unconscious, and they are unable to make his or her own medical decisions in the opinion of the treating physician. As of Jan.1, 2012, all powers of attorney in the state of Arkansas are considered durable unless otherwise stated in the document, so do make special instructions if you wish to choose to have a more limited power, created.
Living Will (Advance Directive) – Allows the patient to enter their end-of-life decisions without the use of an agent or health care surrogate.
State Definition – § 20-6-117(4)
Laws – § 20-6-103(b) & § 20-6-117
How To Write
Download: Adobe PDF
1 – Obtain The PDF Document Here To Issue Health Care Powers In Arkansas
When you are ready to access the document in the preview image, select the “PDF” button or the “Adobe PDF” link on this page. Download this file to an accessible folder on your machine. You may complete this document on screen or print it then fill it out by hand.
2 – The Title And First Paragraph Require Some Preparation
Once you are ready to prepare this document, locate the title. Currently, this title is incomplete. It will require the full name of the individual naming an Attorney-in-Fact to represent and deliver his or her health care directives in the State of Arkansas. This entity is known as the Principal.  Next, record the full name of the Attorney-in-Fact on the first blank space after the statement “Pursuant To The Arkansas Health Care Decisions Act….” The Attorney-in-Fact is the individual that will accept the responsibility and authority of representing the Principal named above.
Next, record the full name of the Attorney-in-Fact on the first blank space after the statement “Pursuant To The Arkansas Health Care Decisions Act….” The Attorney-in-Fact is the individual that will accept the responsibility and authority of representing the Principal named above.  This paperwork will need to include a definitive way to contact the Attorney-in-Fact. Thus, report the Attorney-in-Fact’s telephone number on the second blank space. You may record more than one phone number. If you require more room, you may also cite an attachment with this information.
This paperwork will need to include a definitive way to contact the Attorney-in-Fact. Thus, report the Attorney-in-Fact’s telephone number on the second blank space. You may record more than one phone number. If you require more room, you may also cite an attachment with this information. 
3 – Review Each Power Description Then Determine If You Approve Of Its Appointment
The language required to deliver an Attorney-in-Fact the right to represent your decisions regarding medical treatment to medical staff is set in this document. By default, the Attorney-in-Fact will be granted the power to engage in a wide array of decisions and actions on your behalf. The list following the introduction will summarize these representational powers. You will have to go through this list and cross out or remove each statement describing an action the Attorney-in-Fact should be restricted from taking when representing you. For example, you may not wish the Attorney-in-Fact to be able to deny the administration of a pain management program. In such an example, you would need to cross out statement “(F).” 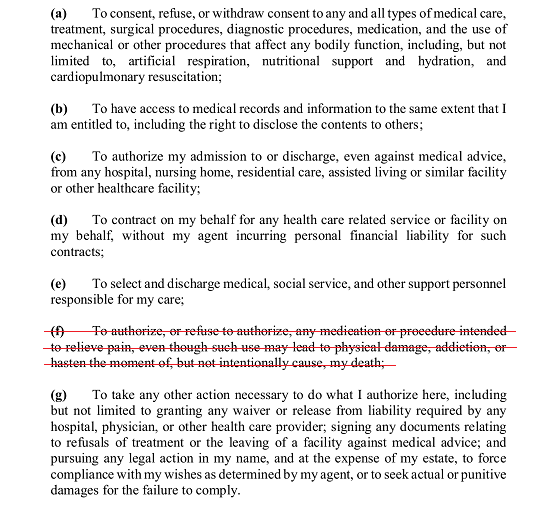 The first subject this list details is consent. If you wish the Attorney-in-Fact to be able to decide whether your consent to medical treatment or intervention should be given, kept in place, withheld, or removed then leave the item labeled “(A)” intact. You may remove this statement or cross it out with a red pen if you do not want the Attorney-in-Fact to have these powers.
The first subject this list details is consent. If you wish the Attorney-in-Fact to be able to decide whether your consent to medical treatment or intervention should be given, kept in place, withheld, or removed then leave the item labeled “(A)” intact. You may remove this statement or cross it out with a red pen if you do not want the Attorney-in-Fact to have these powers.  The second statement delivers access to your medical records and any other medical information to the Attorney-in-Fact. You may leave this statement unaltered to apply it to the Attorney-in-Fact’s rights when representing you or you may delete/strikethrough it if you do not want him or her to have access to your medical information and history.
The second statement delivers access to your medical records and any other medical information to the Attorney-in-Fact. You may leave this statement unaltered to apply it to the Attorney-in-Fact’s rights when representing you or you may delete/strikethrough it if you do not want him or her to have access to your medical information and history.  You can authorize your Attorney-in-Fact to decide upon your stay at a medical facility. Statement “(C)” will give your Attorney-in-Fact the right to decide whether you should be admitted or discharged to a medical facility. This will include the authority to disobey the suggestions of medical personnel as well. Cross this out if you do not wish the Attorney-in-Fact to have this power. If you do approve of the Attorney-in-Fact being able to take such actions on your behalf, then leave this statement unmarked.
You can authorize your Attorney-in-Fact to decide upon your stay at a medical facility. Statement “(C)” will give your Attorney-in-Fact the right to decide whether you should be admitted or discharged to a medical facility. This will include the authority to disobey the suggestions of medical personnel as well. Cross this out if you do not wish the Attorney-in-Fact to have this power. If you do approve of the Attorney-in-Fact being able to take such actions on your behalf, then leave this statement unmarked.  The ability to contract “…Health Care Related Service Or Facility” on your behalf can be granted to the Attorney-in-Fact through the wording in the fourth statement “(D).”
The ability to contract “…Health Care Related Service Or Facility” on your behalf can be granted to the Attorney-in-Fact through the wording in the fourth statement “(D).”
This statement will also absolve your Attorney-in-Fact of any financial liability for such service contacted.  If the Attorney-in-Fact should also have the authority “To Select And Discharge Medical, Social Service, And Other Support Personnel” in your name, then statement “(E)” will grant such power. However, if you wish the Attorney-in-Fact to be restricted from such actions, then cross out or delete this item.
If the Attorney-in-Fact should also have the authority “To Select And Discharge Medical, Social Service, And Other Support Personnel” in your name, then statement “(E)” will grant such power. However, if you wish the Attorney-in-Fact to be restricted from such actions, then cross out or delete this item. ![]() Statement “(F)” delivers the same authority you carry when authorizing or refusing pain management techniques and medications. The ability to make such decisions on your behalf can be withheld from the Attorney-in-Fact if you remove this item or strike through it.
Statement “(F)” delivers the same authority you carry when authorizing or refusing pain management techniques and medications. The ability to make such decisions on your behalf can be withheld from the Attorney-in-Fact if you remove this item or strike through it.  You may have a scenario where additional powers not discussed above should be within the Attorney-in-Fact’s ability when acting in your name. The wording in statement “(G)” will deliver some fairly broad powers of representation to the Attorney-in-Fact if he or she needs “To Take Any Other Action” necessary to carry out the directives you have authorized here. If you wish you may deny such a scope of representational power to the Attorney-in-Fact by deleting or crossing out this statement. Otherwise, leave it unmarked so that it could be included in the principal powers being granted to the Attorney-in-Fact.
You may have a scenario where additional powers not discussed above should be within the Attorney-in-Fact’s ability when acting in your name. The wording in statement “(G)” will deliver some fairly broad powers of representation to the Attorney-in-Fact if he or she needs “To Take Any Other Action” necessary to carry out the directives you have authorized here. If you wish you may deny such a scope of representational power to the Attorney-in-Fact by deleting or crossing out this statement. Otherwise, leave it unmarked so that it could be included in the principal powers being granted to the Attorney-in-Fact. 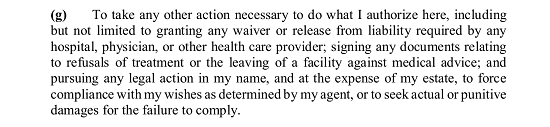 Read the statement after this list very carefully. It would be considered very inadvisable to make any alterations to it without consulting a qualified professional beforehand. This statement will give your Attorney-in-Fact the “…The Authority To Make Decisions About Withholding Or Withdrawal Of Life-Sustaining Treatment, And Nutrition And Hydration…” as you have defined in your Living Hill and/or Advance Care Plan.
Read the statement after this list very carefully. It would be considered very inadvisable to make any alterations to it without consulting a qualified professional beforehand. This statement will give your Attorney-in-Fact the “…The Authority To Make Decisions About Withholding Or Withdrawal Of Life-Sustaining Treatment, And Nutrition And Hydration…” as you have defined in your Living Hill and/or Advance Care Plan. 
4 – You Have The Option To Name Additional Parties To Represent Your Interests
The last paragraph where you will discuss the authority you are granting here will give you the opportunity to name an Alternate Attorney-in-Fact who will automatically be granted the same authority being delivered to the original Attorney-in-Fact. This granting of power will operate in a successive manner, meaning that these two entities are unable to represent you at the same time. Whether you anticipate the original Attorney-in-Fact ever being unable, ineligible, or unwilling to represent you in the future (i.e. he or she is out of the country when you become incapacitate), this is a reasonably good precaution to take. If you wish to name a Successor Attorney-in-Fact for this role, then enter the name of the original Attorney-in-Fact on the first blank line and the name of the intended Successor Attorney-in-Fact on the second blank line to supplement the wording in this paragraph. 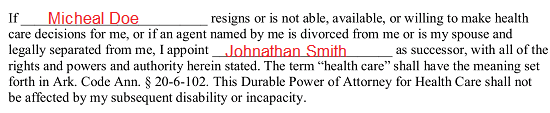 There is one additional option to this document. At times, a Principal who is declared incapacitated may have a Guardian or Conservator appointed by the courts. The last paragraph will allow you to nominate an individual to this role. This option does not guarantee any such nomination is automatically appointed by the courts but often, but such a nomination is usually taken into serious consideration. To nominate an individual to either of these roles, locate the bracketed labels “[Full Name],” “[Full Address],” and “[Phone Number].” Replace each label with the information it calls for.
There is one additional option to this document. At times, a Principal who is declared incapacitated may have a Guardian or Conservator appointed by the courts. The last paragraph will allow you to nominate an individual to this role. This option does not guarantee any such nomination is automatically appointed by the courts but often, but such a nomination is usually taken into serious consideration. To nominate an individual to either of these roles, locate the bracketed labels “[Full Name],” “[Full Address],” and “[Phone Number].” Replace each label with the information it calls for. 
5 – Sign Your Name To This Paperwork To Execute The Granted Authority
Review the information you have supplied to any of the paragraphs in this document. If this information is accurate and you are ready to set the approval for the granted powers as active, you must supply a dated signature that has been witnessed and notarized. Begin this execution process by filling in the current calendar date on the day you are signing this paperwork to the three blank spaces after the words “Signed This…”  Sign your name on the line labeled “Signature.” Make sure this is done before two witnesses and a notary immediately after you have reported the date above.
Sign your name on the line labeled “Signature.” Make sure this is done before two witnesses and a notary immediately after you have reported the date above.  The name of the Principal must be supplied after the word “Declarant” in the next paragraph. This is the statement that each Witness must read then acknowledge as true by signing and printing his or her name on the lines labeled “Print Witness Name” and “Signature Of Witness.” There will be enough room for each witness to perform this action in a unique area.
The name of the Principal must be supplied after the word “Declarant” in the next paragraph. This is the statement that each Witness must read then acknowledge as true by signing and printing his or her name on the lines labeled “Print Witness Name” and “Signature Of Witness.” There will be enough room for each witness to perform this action in a unique area. 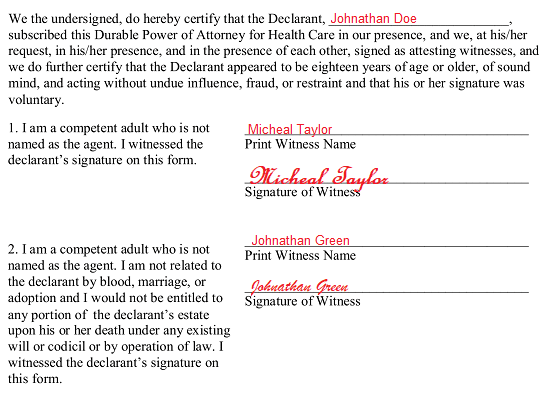 The last page of this document requires participation from a Notary Public. He or she will fill in this page as part of the notarization process.
The last page of this document requires participation from a Notary Public. He or she will fill in this page as part of the notarization process.