 | California Advance Directive Form | Medical POA & Living Will |
The California advance directive is used to choose a health care surrogate to represent your medical decisions and to make decisions about life-sustaining treatment options. The directive is a combination of a Medical Power of Attorney and Living Will. Therefore, the entire form allows the principal to select someone that will have the authorization to make decisions in the chance the principal cannot do so for themselves. In addition, the form allows for the patient to make end-of-life decisions in the chance they become in a state of permanent incapacitation.
Laws – Probate Code § 4701
Advance Directive Registration (Form SFL-461) – At the option of the Principal, they may choose to register the Advance Directive with the State by completing this form, attaching $10, and sending to:
Signing Requirements (Probate Code § 4673(3)) – Two (2) Witnesses OR a Notary Public
How To Write
Download: Adobe PDF
1 – The Adobe File On This Page Should Be Downloaded
You may access the California paperwork to designate an Agent with the authority to be your Health care Representative and/or document health care directives by selecting the link labeled “Adobe (.PDF)” or clicking on the appropriately labeled button.
2 – Name The Individual You Wish To Grant Authority
Read the first page since it will contain information that you must be familiar with before you fill out this form.  If you would like to name a Health Care Representative, then locate the area labeled “Part 1 Power Of Attorney For Health Care.” Use the line below this, “(1.1) Designation Of Agent,” to present the first, middle, and last name of the individual you would like to represent your treatment preferences. Make sure this name appears exactly on this entity’s I.D. papers.
If you would like to name a Health Care Representative, then locate the area labeled “Part 1 Power Of Attorney For Health Care.” Use the line below this, “(1.1) Designation Of Agent,” to present the first, middle, and last name of the individual you would like to represent your treatment preferences. Make sure this name appears exactly on this entity’s I.D. papers.  The second line in this area will contain three blank spaces (“Address,” “City,” “State,” and “Zip Code”). Use these spaces to fill in the building number, street, apartment number, city, state, and zip code where the Attorney-in-Fact you selected lives.
The second line in this area will contain three blank spaces (“Address,” “City,” “State,” and “Zip Code”). Use these spaces to fill in the building number, street, apartment number, city, state, and zip code where the Attorney-in-Fact you selected lives.  Next, report your Attorney-in-Fact’s “Home Phone” number and “Work Phone” number on the next two blank spaces.
Next, report your Attorney-in-Fact’s “Home Phone” number and “Work Phone” number on the next two blank spaces.  The “Optional” paragraph will enable you to name an Alternate Agent. Such an individual would assume the authority you deliver to the Health Care Representative you named above should he or she no longer be able to represent you or unwilling to. This is the only time the Alternate Agent will be authorized to represent you. If you do wish to set such an entity in place then, record his or her name, complete home address, home telephone number, and work telephone number using the appropriately labeled blank lines below the phrase “…As My First Alternate Agent.”
The “Optional” paragraph will enable you to name an Alternate Agent. Such an individual would assume the authority you deliver to the Health Care Representative you named above should he or she no longer be able to represent you or unwilling to. This is the only time the Alternate Agent will be authorized to represent you. If you do wish to set such an entity in place then, record his or her name, complete home address, home telephone number, and work telephone number using the appropriately labeled blank lines below the phrase “…As My First Alternate Agent.” 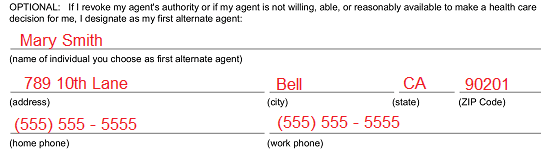 The second “Optional” section will have a similar purpose as the first. Suppose that for some reason both the original Health Care Representative and First Alternate Agent you have named above cannot or will not be able to represent you when you are incapacitated and a medical decision (that you are unable to provide) is required. Only an individual with proof of your approval will be able to take up this role. You may pre-approve a Second Alternate Agent to step into the role of representing you by entering his or her full name, complete address, and contact information (home and work phone numbers) on the spaces presented under the term “…My Second Alternate Agent.”
The second “Optional” section will have a similar purpose as the first. Suppose that for some reason both the original Health Care Representative and First Alternate Agent you have named above cannot or will not be able to represent you when you are incapacitated and a medical decision (that you are unable to provide) is required. Only an individual with proof of your approval will be able to take up this role. You may pre-approve a Second Alternate Agent to step into the role of representing you by entering his or her full name, complete address, and contact information (home and work phone numbers) on the spaces presented under the term “…My Second Alternate Agent.” 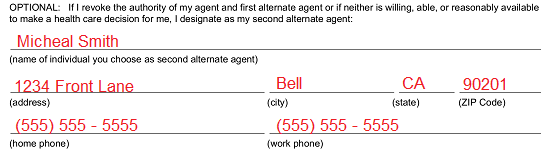
3 – Formally Document The Actions Your Agent May Or May Not Engage In
The statement labeled “(1.2) Agent’s Authority” will give the Agent(s) you named above a wide scope of principal power when it comes to making decisions concerning your treatment options, medical interventions, pain management, and virtually any medical decision. Since this power becomes available to the Agent if you are incapacitated and vulnerable, any limitations you wish imposed upon the Agent’s ability to make health care decisions on your behalf should be recorded on the blank lines provided after the words “…except As I state Here.” You have a certain freedom with the language you use (it can be general or very specific) however make sure the limitations you wish placed are well-defined. If there is not enough room, you may add more space as you go, or you may attach the restrictions as a separate document whose title is presented in this area. 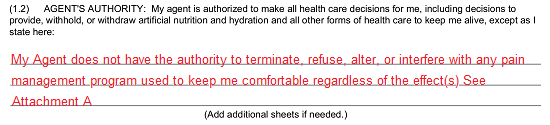
4 – Review The Next Paragraphs And Provide Information Where Requested
You will need to supply a definition as to when the powers you are granting the Health Care Agent will become available to this party. He or she may be authorized to act only if a physician declares you (in writing) as incapacitated or as soon as you sign this document. This will be at your discretion, but you must document this preference before signing this form. You may do so through “(1.3) When Agent’s Authority Becomes Effective.” If the Agent should not have any ability to represent you until a Physician has officially declared, you as incapacitated then leave the language in this statement unaltered. ![]() If you wish your Agent’s authority to become effective as soon as you sign this document, then mark the checkbox preceding the words “My Agent’s Authority To Make Health Care Decisions For Me Takes Effect Immediately” (see example below).
If you wish your Agent’s authority to become effective as soon as you sign this document, then mark the checkbox preceding the words “My Agent’s Authority To Make Health Care Decisions For Me Takes Effect Immediately” (see example below). ![]() The responsibility of the Agent to act according to your instructions will be detailed in “(1.4) Agent’s Obligation.”
The responsibility of the Agent to act according to your instructions will be detailed in “(1.4) Agent’s Obligation.”  By default, your Health Care Agent will have decision making power concerning what should be done with your remains as per “(1.5) Agent’s Postdeath Authority.” You may limit or forbid such authority from being delivered by stating as much on the blank lines provided. If you wish to not limit your Agent’s control over your remains and have no limitations to be set upon such authority then write in the word “None.”
By default, your Health Care Agent will have decision making power concerning what should be done with your remains as per “(1.5) Agent’s Postdeath Authority.” You may limit or forbid such authority from being delivered by stating as much on the blank lines provided. If you wish to not limit your Agent’s control over your remains and have no limitations to be set upon such authority then write in the word “None.”  Statement “(1.6) Nomination Of Conservator” will automatically nominate your Health Care Agent and, if no longer available, your Successor Agents as your Guardian or Conservator should the courts decide one is required in the future. If you do not wish the courts to take any of these entities under consideration for this role then delete or cross out this statement.
Statement “(1.6) Nomination Of Conservator” will automatically nominate your Health Care Agent and, if no longer available, your Successor Agents as your Guardian or Conservator should the courts decide one is required in the future. If you do not wish the courts to take any of these entities under consideration for this role then delete or cross out this statement. ![]()
5 – Document Your Instructions Concerning Traumatic Medical Events And Interventions
“Part 2 Instructions For Health Care” will enable you to document your directives concerning an end-of-life scenario. If you wish to address this issue, you may begin doing so in “(2.1) End-Of-Life Decisions.” This area will present two checkbox statements where you must select one to define how you want such a situation to be handled. If you have determined that you do not want medical staff to intervene when you have been diagnosed with a terminal condition (i.e. an incurable disease) that will result in your death within a short time frame, have been rendered permanently unconscious, or when the only treatment available has great risk and few benefits then, mark the checkbox labeled “(A) Choice Not To Prolong Life.” 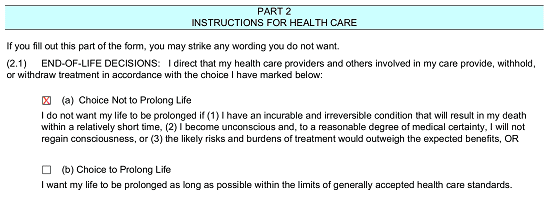 Mark the second checkbox, “(B) Choice To Prolong Life,” if you do wish that medical staff prolong your life with the current acceptable medical treatments/interventions at the time.
Mark the second checkbox, “(B) Choice To Prolong Life,” if you do wish that medical staff prolong your life with the current acceptable medical treatments/interventions at the time. 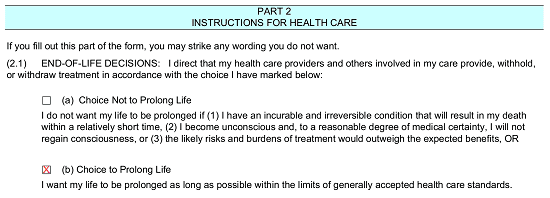 The next statement “(2.2) Relief From Pain” will solidify your need to alleviate pain even at the risk of death. You can provide exceptions to this stance or you may restrict the use of such procedures using the blank lines provided.
The next statement “(2.2) Relief From Pain” will solidify your need to alleviate pain even at the risk of death. You can provide exceptions to this stance or you may restrict the use of such procedures using the blank lines provided.  You can add additional provisions, instructions, limitations, or restrictions concerning end-of-life scenarios directly to this paperwork. If you do wish to provide additional documentation for your directives, then do so using the blank lines in “(2.3) Other Wishes.”
You can add additional provisions, instructions, limitations, or restrictions concerning end-of-life scenarios directly to this paperwork. If you do wish to provide additional documentation for your directives, then do so using the blank lines in “(2.3) Other Wishes.”  In addition to the previous information you have supplied, this template will give you an opportunity to further address what you wish done with your body after death. We will discuss this matter in “Part 3 Donation Of Organs, Tissues, And Parts At Death (Optional).”
In addition to the previous information you have supplied, this template will give you an opportunity to further address what you wish done with your body after death. We will discuss this matter in “Part 3 Donation Of Organs, Tissues, And Parts At Death (Optional).” 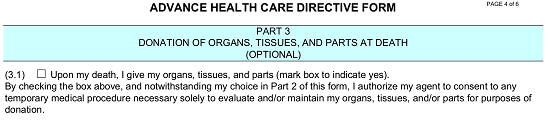 If you would like to donate your “…Organs, Tissues, And Parts…” once you have passed away, then mark the checkbox in “(3.1).” See the example below.
If you would like to donate your “…Organs, Tissues, And Parts…” once you have passed away, then mark the checkbox in “(3.1).” See the example below. 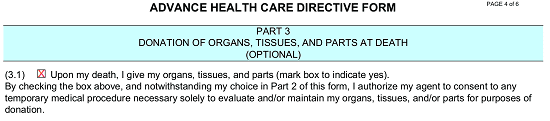 Next, a brief list is presented. This list will cover the various purposes of an organ or tissue donation. If you do not wish any body parts donated for one of these purposes, then cross it out or remove it by deleting it. For example, if you only wish to make an organ donation for “Transplant” or “Therapy” purposes and for no other reason, then cross out “(C) Research” and “(D) Education.” See the example below.
Next, a brief list is presented. This list will cover the various purposes of an organ or tissue donation. If you do not wish any body parts donated for one of these purposes, then cross it out or remove it by deleting it. For example, if you only wish to make an organ donation for “Transplant” or “Therapy” purposes and for no other reason, then cross out “(C) Research” and “(D) Education.” See the example below.  If you have additional restrictions or any specific instructions defining any organ donations made from your remains, they must be documented on the blank line after the statement beginning with the term “If You Want To Restrict…”
If you have additional restrictions or any specific instructions defining any organ donations made from your remains, they must be documented on the blank line after the statement beginning with the term “If You Want To Restrict…” 
6 – Present The Identity And Contact Information For Your Primary Physician
An optional section “Part 4 Primary Physician” has been included at the end of this document. Here, you can document the name of your Primary Physician. This may be a good measure to employ since your Primary Physician has (in most cases) up-to-date information defining your health. Three lines with several blank labeled blank spaces have been provided in this section. Use these spaces to deliver the “Name Of Physician” along with his or her office “Address,” “City,” “State,” “Zip Code,” and “Phone” number. 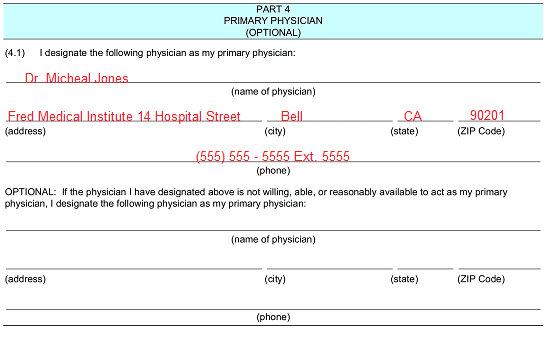 You can name a second Physician to be contacted here, in case the one above is unavailable or unwilling to act in a reasonable amount of time. Several blank spaces labeled “Name Of Physician,” “Address,” “City,” “State,” “Zip Code,” and “Phone” under the “Optional: If The Physician I Have Designated Above Is Not Willing…” statement have been provided to achieve this purpose.
You can name a second Physician to be contacted here, in case the one above is unavailable or unwilling to act in a reasonable amount of time. Several blank spaces labeled “Name Of Physician,” “Address,” “City,” “State,” “Zip Code,” and “Phone” under the “Optional: If The Physician I Have Designated Above Is Not Willing…” statement have been provided to achieve this purpose. 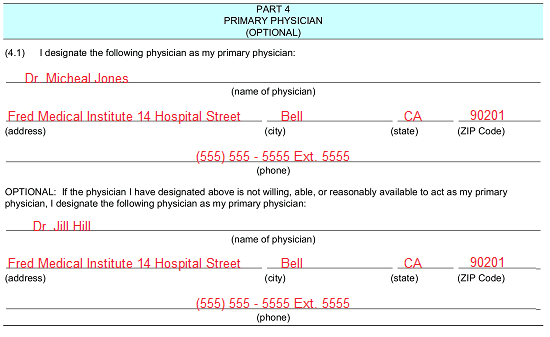
7 – Several Parties And You Must Cooperate To Execute This Paperwork
The final area, “Part 5,” will enable you to finalize the directives you have placed in this document. This can only be done with a verifiable signature that you provide. Locate, the area labeled “(5.2) Signature.” You must fulfill all this section’s requirements at one time before two qualifying Witnesses, so make sure to coordinate with these individuals. First, locate the column of labeled spaces on the left “(Date),” “(Address),” and “(City) (State).” Use these spaces to fill in the calendar date of the day you are signing this paperwork and your residential address. 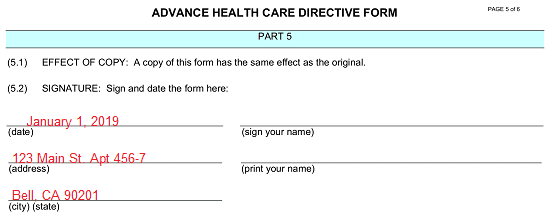 Now that you have supplied these items to the left-hand column, locate the blank spaces “(Sign Your Name)” and “(Print Your Name).” You must supply your signature and printed name to these lines before the designated Witnesses and on the same day as the calendar date you have recorded.
Now that you have supplied these items to the left-hand column, locate the blank spaces “(Sign Your Name)” and “(Print Your Name).” You must supply your signature and printed name to these lines before the designated Witnesses and on the same day as the calendar date you have recorded. 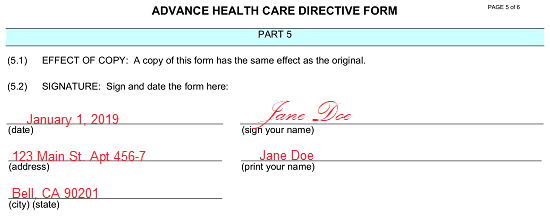 As mentioned earlier, two Witnesses must watch you sign this document. Each one will need to meet the qualifications stated in “(5.3) Statement Of Witnesses.” This means that neither Witness can be named as the Health Care Agent, Successor Agent, not employed or associated with your health care provider/facility/institution responsible for your care and can verify your identity and soundness of mind. If, and only if, the Witnesses will testify to this statement as true, then they must print their names, supply their addresses, sign their names, and report their signature dates to the columns to the “First Witness” and “Second Witness” columns.
As mentioned earlier, two Witnesses must watch you sign this document. Each one will need to meet the qualifications stated in “(5.3) Statement Of Witnesses.” This means that neither Witness can be named as the Health Care Agent, Successor Agent, not employed or associated with your health care provider/facility/institution responsible for your care and can verify your identity and soundness of mind. If, and only if, the Witnesses will testify to this statement as true, then they must print their names, supply their addresses, sign their names, and report their signature dates to the columns to the “First Witness” and “Second Witness” columns. 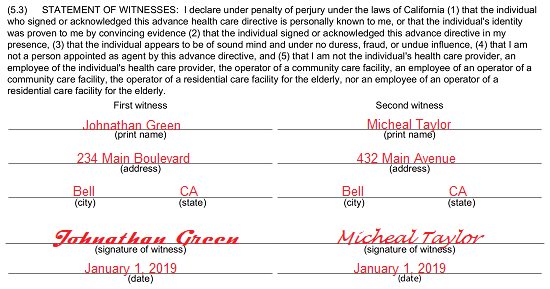 Ideally, both Witnesses must sign the “(5.4) Additional Statement Of Witnesses” statement however, it is acceptable if only one meets the qualifications of this statement. Only a Witness who is not part of your family (wife, blood relative, adoption) can sign this statement. At least one Witness signature is required here, or this document may not be considered a valid representation of your preferences.
Ideally, both Witnesses must sign the “(5.4) Additional Statement Of Witnesses” statement however, it is acceptable if only one meets the qualifications of this statement. Only a Witness who is not part of your family (wife, blood relative, adoption) can sign this statement. At least one Witness signature is required here, or this document may not be considered a valid representation of your preferences.  If one of the Witnesses is a nurse in a skilled nursing facility (that provides care on an extended basis) and can be considered your Patient Advocate Or Ombudsman, then he or she must supply a signature “(Date)” along with his or her “(Address),” “(City)(State),” signature, and printed name to the signature area in “Part 6 Special Witness Requirement.”
If one of the Witnesses is a nurse in a skilled nursing facility (that provides care on an extended basis) and can be considered your Patient Advocate Or Ombudsman, then he or she must supply a signature “(Date)” along with his or her “(Address),” “(City)(State),” signature, and printed name to the signature area in “Part 6 Special Witness Requirement.”