 | Hawaii Medical Power of Attorney Form |
The Hawaii medical power of attorney form is a legal written document created by the Principal with regard to their future medical care. It is a document that will instruct your Attorney In Fact/Agent how you would like your medical care handled so that family members and friends won’t have to guess what you want in the event you are no longer able to offer direction or speak for yourself. This document has been updated as of December of 2015. While the previous advance directive forms are still valid, it’s recommended that you only use this updated document. (See Haw. Rev. Stat. § 327E-16 : Hawaii Statutes – Section 327E-16)
How To Write
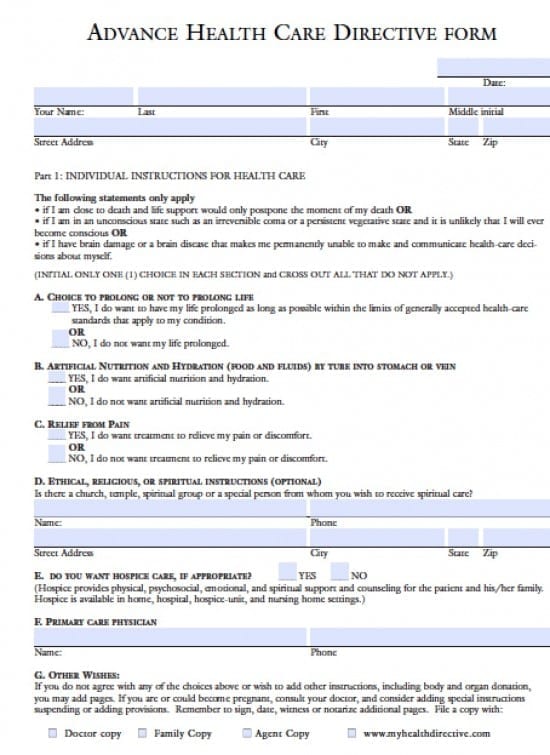
Step 1 – Begin by downloading the document provided and entering the following information:
- Enter the date the Principal is completing the document in mm/dd/yyyy format
- Your (Principal’s) Name
- Last
- First
- Middle initial
- Street Address
- City
- State
- Zip Code
Step 2 – Individual Instructions for Health Care – The Principal must read the statements in this section. Once the statements have been read move to the next section and initial only one selection in sections A through C and strike through the rejected option as follows:
- A. CHOICE TO PROLONG OR NOT TO PROLONG LIFE
- YES, I do want to have my life prolonged as long as possible within the limits of generally accepted health-care standards that apply to my condition.
- OR
- NO, I do not want my life prolonged
- B. ARTIFICIAL NUTRITION AND HYDRATION (FOOD AND FLUIDS) BY TUBE INTO STOMACH OR VEIN
- YES, I do want artificial nutrition and hydration
- OR
- NO, I do not want artificial nutrition and hydration
- C. RELIEF FROM PAIN
- YES, I do want treatment to relieve my pain or discomfort
- OR
- NO, I do not want treatment to relieve my pain or discomfort
- D. ETHICAL, RELIGIOUS, OR SPIRITUAL INSTRUCTIONS (OPTIONAL) – Is there a church, temple, spiritual group or a special person from whom you wish to receive spiritual care? Provide the following information, in this section, on the form, so that they may be contacted for you:
- Name
- Phone
- Street
- Address
- City
- State
- Zip Code
- E. Hospice Care – If the Principal would like to have Hospice Care when it becomes appropriate check “yes” in this section on the form.
- F. On the line provided, enter the name and phone number of your Primary Care Provider
- G. Other Wishes – Read the paragraph in this section and follow the instructions
Step 3 – Agent’s Authority and Obligation – The Principal should read the paragraph in this section. Provide the Agent’s information as follows:
- Name of Agent (Spouse, adult child, friend or other trusted person)
- Relationship
- Street Address
- City
- State
- Zip
- Home Phone
- Work Phone
- Alternate or Successor Agent’s information –
- Name of Alternate Agent (Spouse, adult child, friend or other trusted person)
- Relationship
- Street Address
- City
- State
- Zip
- Home Phone
- Work Phone
Step 4 – With regard to Agent’s Authority – Initial the following on the form as follows:
- My agent may make all health-care decisions for me
- OR
- My agent may make all health-care decisions for me except: (enter any exceptions on the line provided)
- My agent’s authority becomes effective when my primary physician determines that I am unable to make health-care decisions
- OR
- My agent’s authority to make health-care decisions for me takes effect immediately
Step 5 – Witnesses, Signatures, Notarization – Before proceeding, this document must be witnessed by two people, should you choose the witness option – one of your witnesses may not be related in any way, marriage, blood, healthcare provider. You may choose to use witnesses or a notary, not both.
- Principal –
- Name of Principal
- Print Your Full Name
- Your Signature
- Date you’re signing this document in mm/dd/yyyy format
- AND
- If choosing witnesses as opposed to a notary provide the following:
- Witness #1 and 2
- Print Name
- Witness Signature
- Date of signature
- Address
- City
- State
- Zip Code
- If you choose to use a notary they must be present prior to the Principal signing the document –
- The notary will complete the document by providing all of the required information and affixing the notary seal
- Make copies for anyone who signs the documents as well as your physicians, insurance companies and any other parties for which the Principal would have interest