 | Massachusetts Medical Power of Attorney Form |
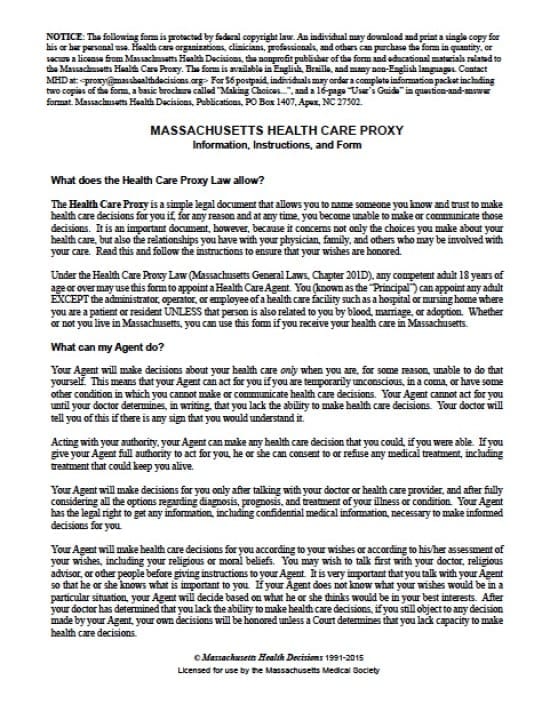
The Massachusetts medical power of attorney form is a legal document that would allow a Principal to appoint an Agent that they would trust, to make health care decisions on their behalf in the event, for any reason, the Principal should become unable to make or communicate their own health care decisions. Due to the fact that this document concerns not only the choices the Principal would choose to make make over their own health care, as well the relationships the Principal would have with their family, physician or anyone else who may be involved with the Principal’s health care. The document should be carefully reviewed by the Principal to ensure that they understand the document they are signing. If it’s unclear, the Principal may wish to contact and consult with an attorney to answer any question for them prior to signing the document.
The Principal may revoke this document at their discretion, This document will require that two (2) witnesses are present to witness the Principal’s signing of the document.
How to Write
Step 1 – Download the document – The Principal must read through the titled sections as follows:
- What does the Health Care Proxy Law allow?
- What can my Agent do?
- Who should have the original and copies?
- How can I revoke or cancel the document?
Step 2 – The Parties –
- In the top right corner, enter the Principal’ date of birth in mm/dd/yyyy format
- Print the name of the Principal
- Enter the Address
- City
- State
- Zip Code
- AND
- Agent’s name
- Street address
- City
- State
- Zip Code
- Telephone number
- Home Phone
- Work Phone
- Email address
- AND
In the event the original agent can no longer serve –
- Alternate Agent’s name (optional)
- Street Address
- City
- State
- Zip Code
- Telephone Number
Step 3 – Exceptions –
- Should the Principal wish to impose limitations or exceptions, type or write them into the space provided
Step 4 – Signatures –
- Signature of Principal
- Date signature in mm/dd/yyyy format
- In the event the Principal is unable to sign the document enter the information regarding who is signing on the Principal’s behalf
- Name of the signatory
- Street Address
- City
- State
- Zip Code
Step 5 – Witness Statements – Each witness must read the statement. If in agreement, each agent must enter:
- Witnesses Signatures
- Witnesses Printed Names
- Full Physical Address
Step 6 – Statements of Health Care Agent and Alternate Agent (Optional) – Both the Agent and Alternate Agent must read their respective paragraphs and provide:
- Signature of Health Care Agent
- Signature of Alternate Agent
Related Forms
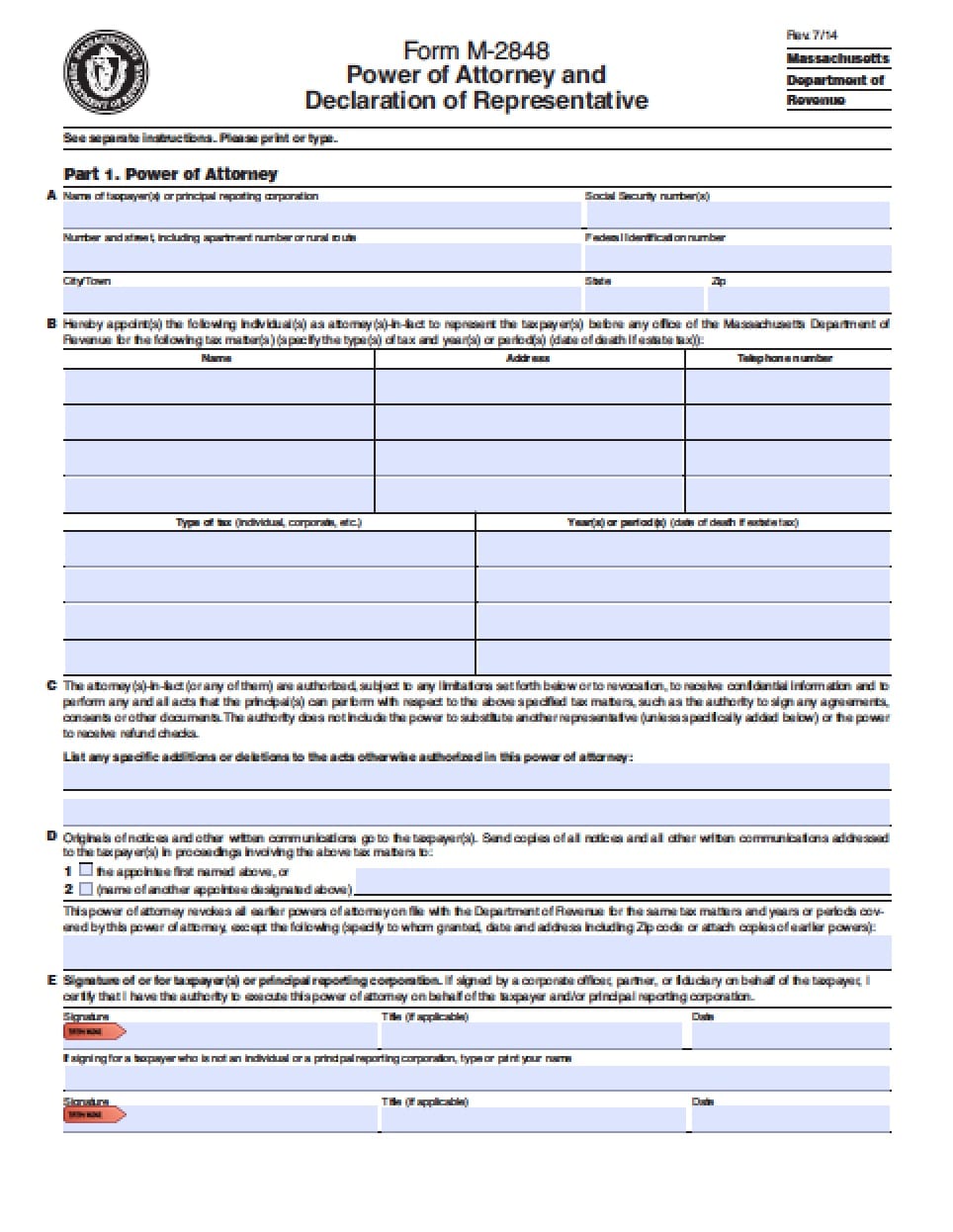 Massachusetts Tax Power of Attorney Form
Massachusetts Tax Power of Attorney Form
 Massachusetts Limited (Special) Power of Attorney Form
Massachusetts Limited (Special) Power of Attorney Form
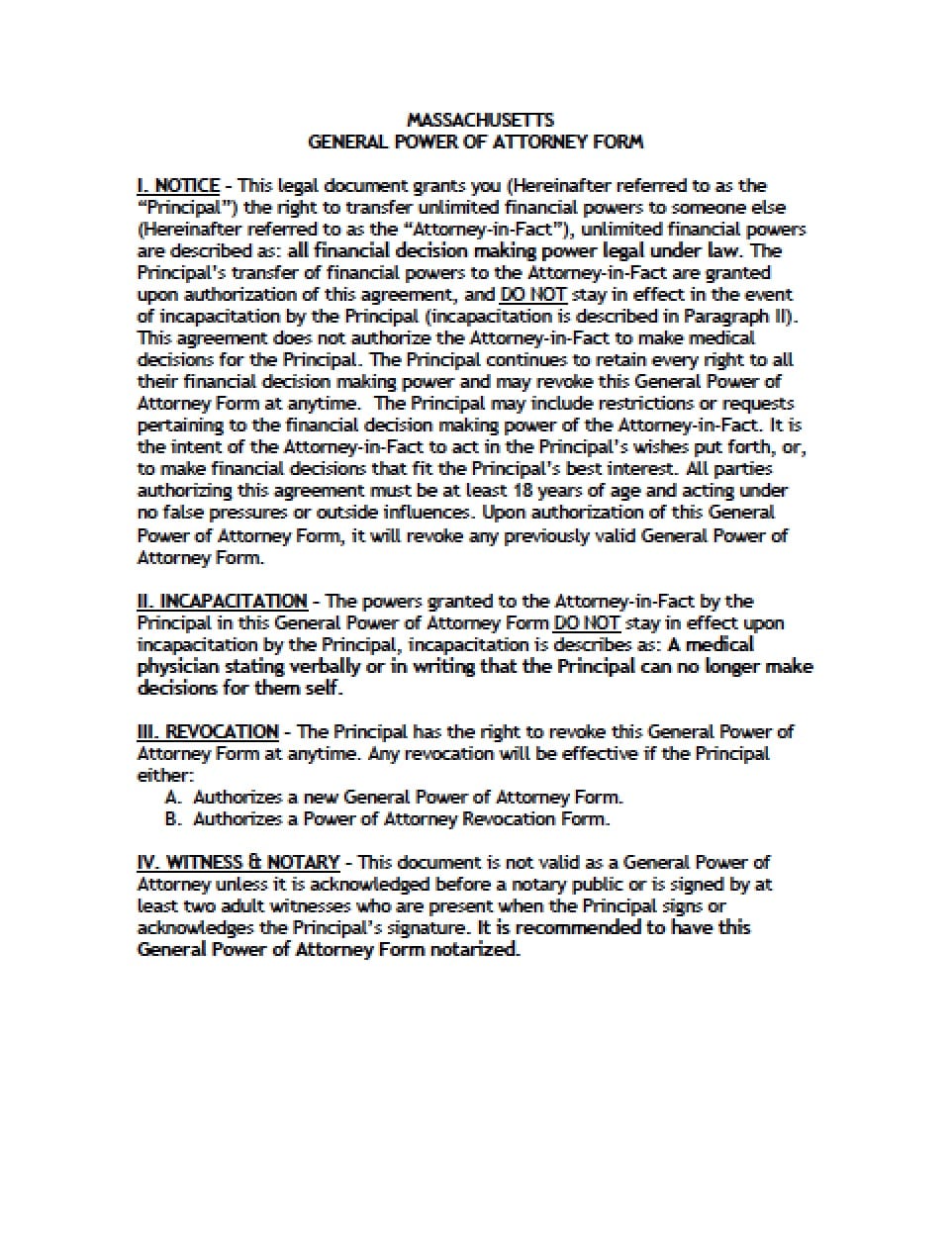 Massachusetts General Financial Power of Attorney Form
Massachusetts General Financial Power of Attorney Form
 Massachusetts Minor Child Power of Attorney Form
Massachusetts Minor Child Power of Attorney Form
 Massachusetts Revocation Power of Attorney Form
Massachusetts Revocation Power of Attorney Form
 Massachusetts Real Estate ONLY Power of Attorney Form
Massachusetts Real Estate ONLY Power of Attorney Form