 | Free Wisconsin Medical Power of Attorney Form |
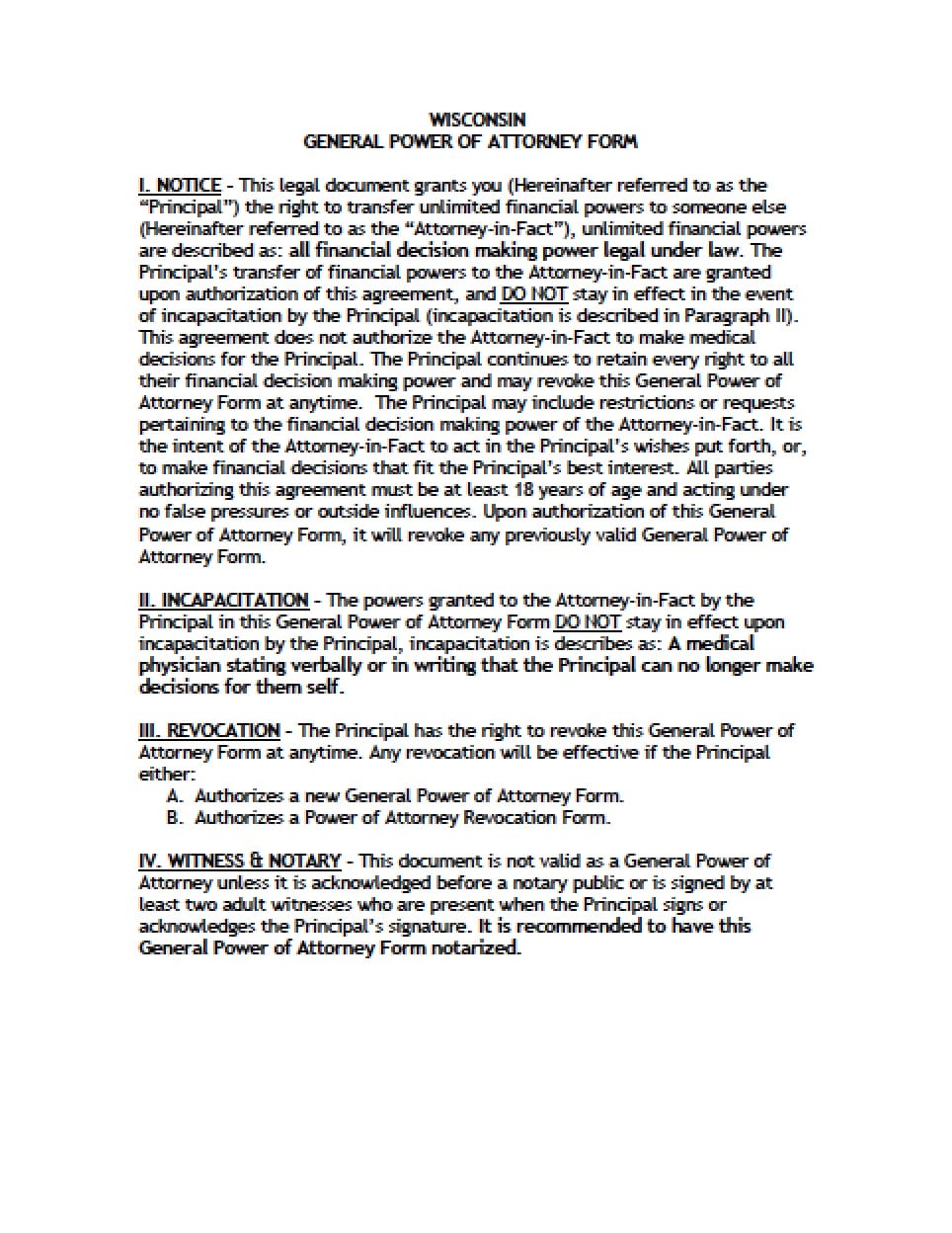
The Wisconsin medical power of attorney form is a document that is created by a Principal for the purpose of delegating powers to an Agent, to make health care decision on behalf of the Principal. The Principal would have the ability to remain in complete control of their health care decisions, unless or until they are no longer able to express or communicate their own directives. If the Principal is uncertain regarding the language of the form, they may consider a consultation with an attorney, prior to completion. This document will not grant powers to act with regard to any of the Principal’s financials or property. This document must be attested by two witnesses. The document may be revoked, by the Principal at any time.
How to Write
Step 1 – Powers Information –
- Download the document and review the first three (3) pages of information
Step 2 – Establishment of Powers – Enter:
- Date of the document in dd/m/yy format
Step 3 – Parties – Submit the following information:
- In the lines provided, enter:
- Principal’s printed name
- Complete physical address
- Date of Birth in mm/dd/yyyy format
- Review the remainder of this section
Step 4 – Designation of Agent – Provide:
- The name of the designated Agent
- Printed name
- Complete Address
- Telephone number
- AND
- The name of a Successor Agent
- Printed name
- Complete address
- Telephone number
- Read “General Statement of Authority Granted”
- AND
- Limitations on Mental Health Treatment
Step 5 – Admission to Nursing Homes or Residential Facilities –
- Check the applicable boxes
Step 6 – Provision of Feeding Tube –
- Read this section
- Check the applicable box indicating the Principal’s choice
Step 7 – Statement of Special Provisions or Limitations – Submit:
- The Principal may specify any special provisions
- Specify any limitations
Step 8 – Signatures – All signatories must be present:
- Principal’s signature
- Date signature in mm/dd/yyyy format
Step 9 – Statement of Witnesses – Witnesses must read and agree to the statement:
- Witnesses printed names
- Date signatures in mm/dd/yyyy format
- Address
- Witness signatures (respective)
Step 10 – Statement of Agent and Successor Agent – Submit:
- Review the statement
- Principal’s name
- Enter the name of the primary Agent
- Both Agents must provide signatures
- Agents addresses
- Read the remainder of the section
Step 12 – Anatomical Gifts (Optional) –
- Check the box that would best indicate the Principal’s gifting preferences (if any)
- Enter any required, additional information
- Principal’s signature
- Date signature in mm/dd/yyyy format