 | Iowa Medical Power of Attorney Form |
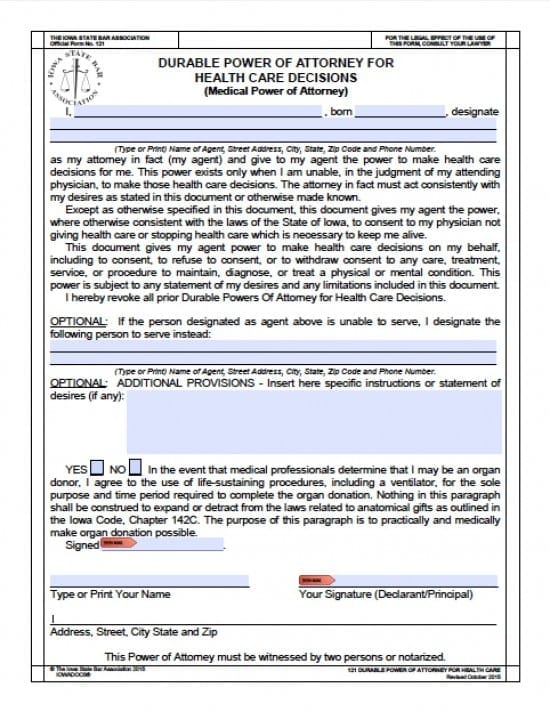
The Iowa medical power of attorney form is a document that allows a Principal to delegate an Agent to oversee the health care of the Principal. The document gives Agent the power to work along with the Principal’s Doctor to make proper health care decisions according to the Principal’s known wishes. The Agent should may be limited or expansive. The decisions will be stated in the document by the Principal. Completion of this form will immediately invalidate any other power’s documents.
This document must be witnessed by two persons OR notarized
How to Write
Step 1 – The Parties –
- Enter the name of the Principal
- Provide the Principal’s Date of Birth
- AND
- Enter the name of the selected Agent
- Enter by type or print
- Agent’s Complete Address
- Telephone Number
- The Principal must review the next paragraphs before proceding
- AND
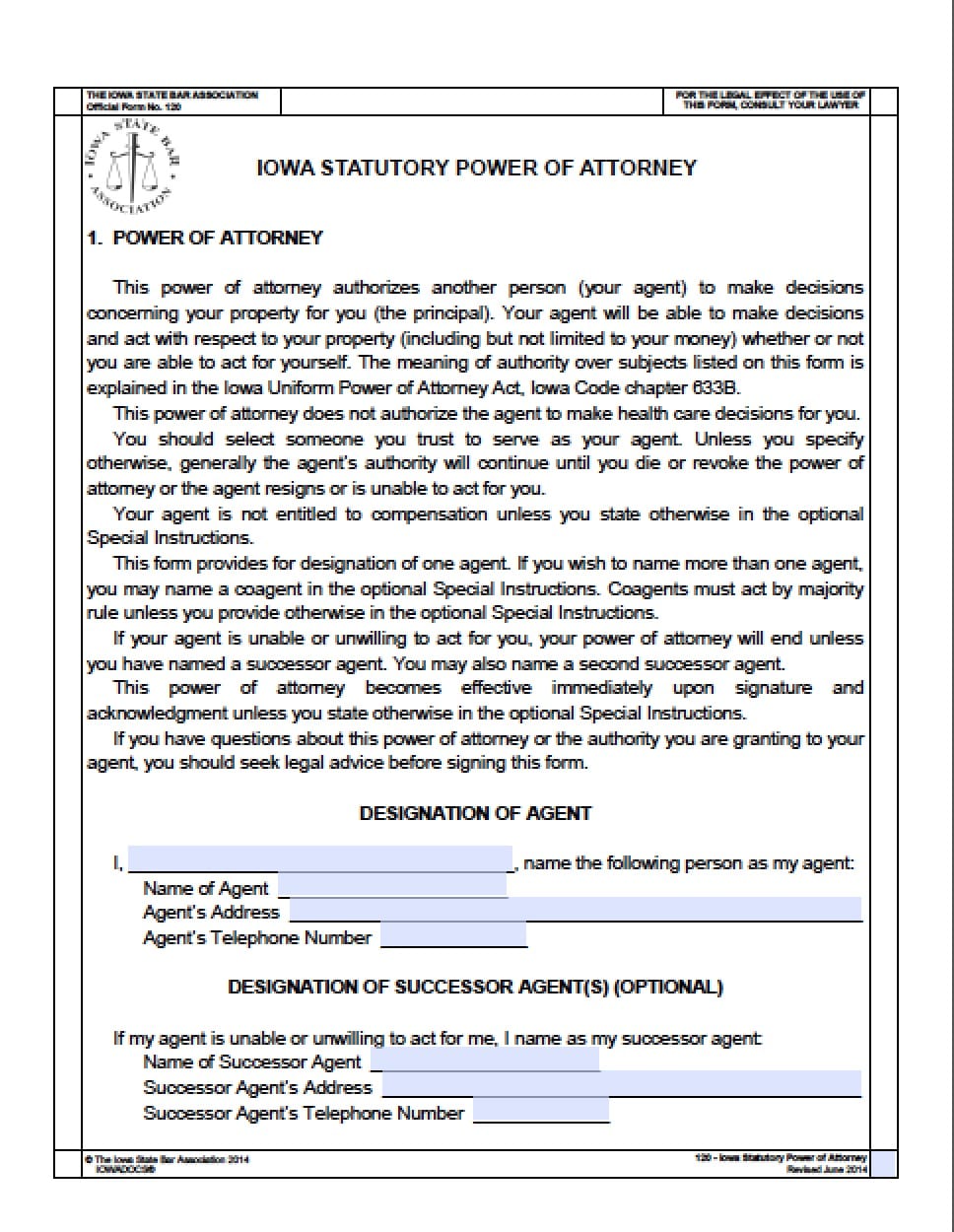
- If the Principal choose, they may select a Successor Agent to step in, in the event the initial Agent should find they are unwilling or unable to serve
- Enter the Successor’s complete address
- Telephone Number
Step 2 – Additional Provisions –
- Should the Principal choose, in the space inside this section, the Principal may specify instructions, and state any specific wishes and desires (if any)
- Check Yes or No regarding whether or not the Principal is willing to provide directives to their Doctor and Agent regarding organ donation
- In order to make it possible for Doctor’s to harvest organs at the end of the Principal’s life, the Principal should enter their signature
- Type or Print the Principal’s Name
- Principal’s Signature
- Address
- Street Address
- City
- State
- Zip Code
Step 3 – Notary Acknowledgment –
- Once the form is completed, the Notary Public, will then enter their information and shall witness all signatures
Step 4 – Witness Form – Complete the following:
- Both Witnesses must review the document
- Provide their respective signatures
- Typed or printed name(s)
- Addresses
- City
- State
- Zip Code
Step 5 – Authorization for Release of Protected Health Information
- Date the document in mm/dd/yyyy format
- Read the Authorization
- If the Principal wishes to have specifically protected information released place an “X” or check any of the boxes regarding the information you would like to release
- Enter the Principal’s Signature
- Date the Signature in mm/dd/yyyy format
Step 6 – Authority to Act as Personal Representative
- Both the Agent and the Principal Should thoroughly review this section
- Date the Signature in mm/dd/yyyy format
- Enter the Principal’s Signature in the line marked “Declarant”
Step 7 – Read all of the information provided under “General Information…” and “Suggestions After Form is Properly Signed, Witnessed and Notarized”