 | Minnesota Medical Power of Attorney Form |
The Minnesota medical power of attorney form is a document that will be created by the Principal, addressing their health care wishes and how the Principal would like to have the wishes carried out. The Principal would then designate an Agent that will properly execute the specific, written instructions that the Principal has set fourth. The Agent will not have the ability to access any of the Principal’s financial accounts.
The document will go into effect when the Principal is no longer able to communicate their own decisions to their health care providers. The Agent must then be prepared to advocate, taking into consideration, with the best intent, the desires of the Principal with regard to their health care. This document provides the ability for the Principal to personalize their decisions and how they will work. The Agent will be fully expected to follow that lead.
This document must be signed before a notary public or two witnesses. The Principal may revoke the form at their discretion.
How to Write
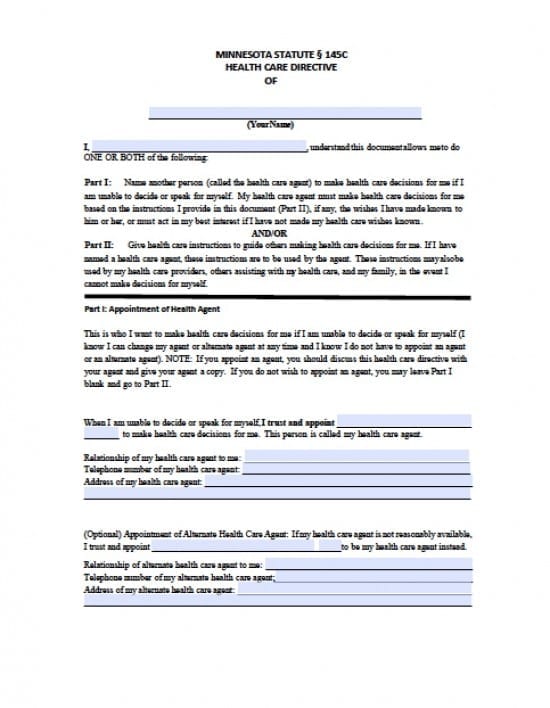
Step 1 – Establish the Principal –
- Enter the full name of the Principal
- In the second line of the document, also, enter the full name of the Principal
- The Principal must read the remaining paragraphs addressing the Principals choices regarding the Agent’s powers
Step 2 – Appointment of Health Agent – The Principal may elect and Agent or could elect to simply state their decisions with no Agent. If an Agent should be selected enter:
- The name of the designated Agent
- The relationship of the Agent to the Principal
- Telephone Number of the Agent
- Full address of the Agent
Step 3 – Appointment of Alternate Agent – If, for some reason the initially selected Agent is unavailable: (optional)
- Enter the name of the Alternate Agent
- Provide the relationship of the Alternate to the Principal
- Enter the Alternate’s Telephone Number
- Provide the address of the Alternate Agent
Step 4 – Principal’s Health Care Expectations of the Agent –
- Review paragraphs A through D
- Should the Principal choose not to utilize the assistance of one or more of the powers listed, limiting the powers granted, enter an explanation in the lines provided
Step 5 – Organ Donation and Disposition of the Principal’s Remains –
- The powers Stated in this section are not automatic powers
- The Principal must initial the statement or both statements that would best fit the wishes of the Agent. Until at least one of these statements are initialed, the powers will not be granted
- Should the Principal have any other decisions with this regard, they may specifically state them in the lines provided
Step 6 – Special Instruction For the Selected Agent and/or Health Care Providers – Enter the Principal’s choices in the lines provided under each health care subject as follows:
- My goals for my health care
- My fears about my health care
- My spiritual or religious beliefs and traditions
- My beliefs about when life would be no longer worth living
- .My thoughts about how my .medical condition might affect my family
- My thoughts about how my health care should be handled in the event I am pregnant
Step 7 – Do’s and Don’ts – This section will address what the Principal wants and does not want included in their health care preferences. Any of these selections may be changed at any time only by the Principal – Read the statements and expand on them:
- If I had a reasonable chance of recovery, and were temporarily unable to decide or speak for myself, I would want
- If I were dying and unable to decide or speak for myself, I would want
- If I were permanently unconscious and unable to decide or speak for myself, I would want
- If I were completely dependent on others for my care and unable to decide or speak for myself, I would want
- In all circumstances, my doctors will try to keep me comfortable and reduce my pain . This is how I feel about pain relief if it would affect my alertness or if it could shorten my life
Principal’s Additional Choices –
- Who I would like to be my doctor
- Where I would like to live to receive health care
- Where I would like to die and other wishes I have about dying
- My wishes about donating parts of my body when I die
- My wishes about what happens to my body when I die (cremation, burial
- Any other things
Step 8 – Signatures – Must be signed before a licensed Notary Public –
- The Principal must read the statements and then provide their signature if they are in agreement
- Date of Principal’s signature in mm/dd/yyyy format
- Date of birth in mm/dd/yyyy format
- The Principal’s Address
- If the Principal has chosen someone to sign in their stead, in the event they are unable to provide signature on their own, then they must have the person they have selected to sign on their behalf, sign the document
- The person who is signing on behalf of the Principal, must also provide their printed name
Step 9 – Notarization –
Once the document has been completed, the notary must witness all of the signatories signatures. The Notary Public shall then provide the necessary Notary information so that they may properly acknowledge the document
Step 10 – Witnesses – Should the Principal choose to use witnesses as opposed to using a Notary, provide the following:
- Both Witnesses must first date their signatures in mm/dd/yyyy format
- Both Witnesses must type or print their name
- Read the information provided regarding witness signatures
- Both Witnesses must enter their signatures
- Both Witnesses must enter their complete addresses
The Principal should provide copies of the document to all signatories as well as other interested parties (ie: health care providers, hospice team, nursing facility etc) The Principal must retain the original copy for record keeping